From 19 days off work to $40,000 in bills, workers on fertility journey need support — and employers are lacking, finds report

More than eight in 10 (82 per cent) employees undergoing fertility treatment took time off work for it — for an average of 18.7 days — drawing on sick days, vacation time, paid or unpaid leave and banked hours.
A further 65 per cent said their fertility journey negatively impacted their employment.
These are some of the findings in a new report from Mount Royal University, conducted in partnership with Fertility Alberta, based on focus groups and a survey of Albertans who underwent fertility care.
“For people who have had long journeys, the emotional, physical and financial pressures that are associated with undergoing especially a prolonged fertility care journey are substantial,” says Rachael Pettigrew, professor and chair of general management and the human resources department at the Bissett School of Business at Mount Royal University.
The report highlights the significant gap in employer support, calling for empathetic policies, benefits and flexibility to ensure employees can cope better at work during a challenging time.
Costly care adds up
The needs are obvious: Respondents reported spending a cumulative average of roughly $35,000 out-of-pocket on fertility care, with an additional average of about $7,000 on related costs such as travel, acupuncture, counselling and legal fees.
And 61 per cent required outside financial assistance — loans or gifts from family and friends — to cover treatment costs.
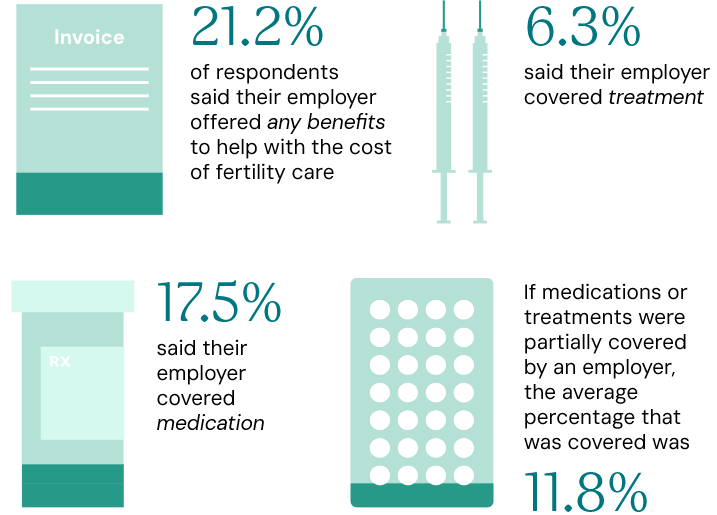
Despite that burden, employer support was scarce: only 21.2% of respondents said their employer offered any kind of benefits to help with fertility care costs. Of those, 6.3% said their employer covered treatment and 17.5% said medications were covered.
Where partial coverage existed, employers were covering an average of 11.8% of costs.
The disclosure dilemma of fertility journey
One of the notable themes to emerge from the research is the burden employees carry when they can't — or won't — tell their employer what they're going through.
The decision about whether to disclose puts employees in a tough position, says Pettigrew. For example, if someone is leaving every other morning over two weeks for an ultrasound to identify if it's an appropriate time for egg retrieval, they are facing a lot of work interruption.
"They’re in a real pickle because if they disclose to their employer, they might actually face some bias that might ‘mommy track’ them,” she says. "There's no guarantee that they'll ever have a successful pregnancy. And then if you don't disclose, you might take vacation for that two-week window, but then you're returning from vacation and it might be the very day you find out that those treatments haven't been successful."
People undergo fertility care for a variety of reasons, she says such as preserving their fertility so they can “lean into work” and have children later, because of cancer treatments or because there are fertility concerns, says Pettigrew.
But the emotional cost of staying silent is substantial.
"One of the participants said that at times they felt like they were leading a double life because they had this big thing happening in their personal life, but their workplace wasn't a safe place to disclose," says Pettigrew. "It adds that emotional labour of having to be hypervigilant about what you say and come up with excuses."
Positive supportive workplace cultures are integral because they create an environment where an employee can disclose what's going on, she says, “and feel confident that they have the psychological safety that if they disclose, that information will be handled well and they won't face repercussions.”
‘It’s very personal’
A lot of employees who may be going through fertility challenges and don't have employer coverage may not want to disclose their situation, agrees Ashley Eberle, a talent acquisition advisor at Alberta Health Services.
Having gone through her own fertility journey before having a daughter, she says “shame” plays a powerful role in keeping employees silent.
“I know a lot of people are still not open to it. I had gone through my journey 10 years before we had our daughter, and I was very secretive about it for the first six years,” says Eberle, who volunteers for Fertility Alberta.
"You don't want people to know what's going on. It's very personal, it's very emotional when you're going through it… you don’t want people asking questions — it puts a lot of pressure on you.”
The disclosure challenge is even more acute for employees in rural and remote areas, who may have little choice but to reveal what's going on, says Pettigrew.
"Their work interruptions are days rather than hours — because they're having to travel off an island or leave a remote community in order to fly somewhere.”
What ‘supportive’ actually means
In the report, 39% of respondents described their workplace culture as supportive of this journey. Flexibility for unpredictable appointments is at the heart of what "supportive" means to employees going through treatment, according to Pettigrew.
"Support is managers being supportive, managers understanding what's going on. It's offering flexibility,” she says.
“Someone might do one round of IVF, get pregnant, and then their journey is done, and it's this very discreet, short-term thing. For others, it's this very ongoing, long process.”
Eberle says that financial coverage and workplace flexibility are equally important pieces of the puzzle. She points to the City of Calgary as one example of an employer whose coverage has become a meaningful differentiator.
The municipality’s benefits booklet says it offers reimbursements for fertility medical services such as:
- physician services’ fees
- diagnostic testing, medical imaging, laboratory and genetic testing
- cryopreservation and services related to sperm retrieval, selection, testing, washing, and preparation
- artificial insemination (AI), Intrauterine insemination (IU), In-vitro fertilization (IVF), assisted h
- atching,
- intra-cytoplasmic sperm injection (ICSI), In-vitro maturation.
"If [people] knew that $40,000 was going to be covered for them versus having to remortgage their house, that's a very big, life-changing decision,” says Eberle.
Business case for fertility coverage
Employers weighing the cost of adding fertility benefits may want to consider both the usage rates and what's at stake if they don't.
"I believe it's about 3% that would actually use the benefits — but that's a huge impact for those 3%,” says Eberle. “It doesn't affect too many people, but the effects of it are huge.”
She adds that the cost of adding fertility benefits to a plan is often less than employers expect: "Once an employer can start asking those questions and costing it out, the pros weigh out way more than the cons."
From a retention standpoint, Pettigrew frames the issue in terms of organizational culture.
"If we can create an organizational culture where people feel supported for this subgroup of our employees who are going through fertility care, my guess is that we're going to be developing a culture that's supportive of someone else's neurodivergence or someone else's work-life balance challenges with their children or aging parents," she says.
"When employees feel supported, there's less attrition [and] it lowers our training costs when people don't leave as often."
Pettigrew also makes the case from a recruitment angle.
"When people are looking on websites or asking about companies to say, 'Oh, this employer has X amount toward fertility care, or even better prescription drug coverage,’ that's attractive to people,” she says.
“If we're going to stick our head in the sand and say… ‘This issue isn't happening for employees,’ then we're probably not going to recruit as effectively as other employers who are offering better policies.”
And with demographics shifting, the window for action may be narrowing.
"The largest proportion of our labour market are baby boomers and they're leaving the workforce," says Pettigrew. "We need to be really strategic with… how we're drawing in younger folks. And if it feels like a sellers’ market right now, I don't think it will be for long."
What meaningful coverage looks like
The average age of first-time mothers in Canada has crept toward 32 and is still climbing, says Eberle — putting more women close to the age threshold at which fertility begins to significantly decline.
"If they're saying 35 years old is the cut-off for your eggs, that's pretty close," she says. "Things are definitely changing and I'm sure we'll see more and more of this come up."
On the coverage side, medication alone can run $5,000 to $6,000 per cycle, and IVF treatment typically costs around $12,000 per round — with most patients requiring one to two rounds, according to Eberle.
Pettigrew says employers don't have to start with full coverage to make a meaningful difference. Entry points might include flexible sick or personal days, enhanced prescription drug coverage, and surveying employees directly to understand what supports they value most.
Diversity in fertility
She also stresses that any fertility policies must be written with inclusivity in mind. Diagnosed infertility is roughly split between men and women, yet policies are often built around female employees. Coverage structures can also create unintended gaps for LGBTQ+ employees.
"Some insurance companies will require a diagnosed infertility in order to cover some of the costs. In a two-mom couple, for example, there may not be diagnosed infertility — it just might be that neither partner has sperm to contribute to the situation; and the same with a two-dad family. So, that immediately means they have less coverage than any other family," says Pettigrew.
She recommends bringing a diverse group of people into the room when drafting policies, and points to specialized platforms — including Carrot Fertility, Progyny Canada and Sprout Family — as resources for employers navigating their options.
"There might be an upfront cost to really meet the needs of key employees, but the flip side will be better recruitment, better retention and a decrease in attrition and overall lower stress for the workforce going through this.”